
|
The best form of treatment is prevention. Many of my clients fall victim to pain and dysfunction because they missed the warning signs.  Don't miss the warning signs! Warning Signs Signs (without symptoms) act as a warning that something bad is about to happen. When I assess movement in my clients (or when I assess my own movement to prevent injuries) I look for signs that are abnormal. To do this, I must know what normal is for athletes and non-athletes. For example, a non-athlete may expect to have glenohumeral (shoulder) external rotation of 80-90 degrees. A baseball player may have as much as 135 degrees on their throwing arm. Some examples of objective signs may include changes (over the last week(s) / month(s) / year(s) in: (1) Range of motion (ROM) Has there been a change in your active or passive ROM? Does the end-feel of the last few degrees of your ROM feel the same as it always has? (i.e. does it feel like a muscle stretch, bone-on-bone, tissue approximation? (2) Coordination Can you perform simple and complex movement skills as easily as before? Are your movements performed with precision? (3) Strength Have you noticed any changes in your ability to access your muscle strength, endurance or power? (4) Speed Are you able to move as quickly in different movement patterns as before? Do you fatigue more easily? (5) Symmetry Are you able to control the left side of your body as well as you are on the right? Do your movements look symmetrical on both sides when you perform them in front of a mirror? Some examples of subjective signs may include: (1) Lack of confidence Do you feel an incapability to execute the skill well? Does something just feel "off"? The skill may look well coordinated but may just feel uncoordinated. (2) Poor decision-making when performing a skill Are you able to make tactical decisions about using the skill? While performing a skill, are you able to make decisions regarding your environment to determine what your next course of action should be? (3) Inability to multitask Do you find it more difficult to talk (or do any number of other skill-sets) while you perform a skill? (4) Poor body language Do you feel awkward performing a skill that you used to be proficient in performing? Do other people seem to smile or chuckle while you perform the skill? (5) Validated outcome measures These outcome measures may help provide the patient with some insight into tasks they perform in their life that are difficult for them to do, even if they do not perceive symptoms to be present. This helps to create self-awareness. (Outcome measure examples include: Roland Morris Disability Questionnaire, Upper Extremity Functional Scale, Upper Extremity Functional Scale, etc.) Onset of Symptoms Once you develop symptoms (e.g. pain, stiffness, numbness, burning, tingling, etc.), we need to take it seriously. I am not implying that you need to take a month off of work, but conversely, the solution is not to ignore the pain and work through it. As always, the healthiest option is found somewhere in the middle. Your liberation from the symptoms will result from: (1) Determining the root cause of the injury. (2) Fixing the problem before permanent damage occurs. (3) Learning from it and becoming more aware of your body. (4) Developing more strength and coordination than before to prevent a similar injury from reoccurring. (5) Gradual return to the sports / activities you enjoy. Concluding Remarks The fundamental process to preventing injuries in your body is being self-aware and having others around you that can point out changes from your baseline. If these do not suffice, or you wish to have more guidance, many experienced physiotherapists are able to assess your movement and create a plan to mitigate your risk factors for future injury. Check out this post for more information on preventative physiotherapy.
1 Comment
When it comes to exercising, there are a lot of choices to be made; How often do I work out? Which body parts should I exercise? How much cardio, core, stretching, etc.. etc.. should I do? How many sets/reps/minutes? The list goes on and on… I’m about to make the exercise selection part of your workout a bit easier. The following list describes 7 exercises that are best left OUT of your work out. Read and enjoy! If you have any comments or questions feel free to leave them in the comment section or contact me personally! 1) Behind The Head Lat Pull Down  This is a great exercise to focus on mid and lower trap development as well as general lat development. You’ll see some of the strongest body builders in the gym doing it, and I only hope that they know it may be harming their neck and shoulders. Because of the head forward (neck protraction) position, you are likely to see muscles like the sternocleidomastoid (SCM), levator scapulae, and upper fibers of the trapezius (traps) tighten up. These muscles are common sources of neck pain, reducing functional neck range of motion, as well as encouraging scapular downward rotation, which can create or further exacerbate shoulder dysfunctions. Additionally, the position of extreme horizontal abduction and external rotation of the shoulder can cause a host of problems that are not limited to shoulder impingement syndrome, rotator cuff strains, labral irritation/tears, AC Joint compression, and ligamentous laxity. 2) Upright Row  The upright row focuses on strengthening the middle and posterior delts, rhomboids and upper traps. It can certainly achieve this goal, however it comes with the risk of shoulder impingement. I personally do not recommend this exercise to many people, but if I do it is always with the limitation of not bringing the elbows up above the shoulder level (as seen in the above picture). 3) Traditional Sit-ups, Crunches and Machines that Simulate Sit-ups Stuart McGill would die and then roll over in his grave if I didn’t mention these exercises. Essentially, yes, these exercises can pack on some muscle and definition to the rectus abdominua, iliopsoas, rectus femoris, and the obliques… However to include these exercises in a regular exercise program is not worth the risk of injury. Going back to basics for a moment- the core is essentially meant to create spinal stability. Another way for me to say this is that the core musculature is meant to functionally operate as an anti-mover for the spine, contracting isometrically. When you do a sit-up you are concentrically contracting the anterior core muscles. Additionally, Stu McGill’s research shows that each intervertebral disc in the lumbar spine has a finite number of spine bends (flexion) that it can tolerate. Due to the structure of the discs, repeated flexion (think rounding the back) is one of the worst motions for lumbar spine health. Crunches, sit-ups, and most abdominal machines in the gym FLEX the spine! So ..stop it!.. and stick to planks, and other exercises that keep the back in a neutral stable position. 4) Leg Press  I love the fact that you can really load up this machine and focus on leg strength, however there are three main flaws I see to using it: 1) The back and feet are planted and impacts the proper knee arthrokinematics (the movement of the joint surfaces) of the tibiofemoral joint to take place. Typically as you straighten the knee, there is a conjunction external rotation of the tibia on the femur. It is hypothesized that this machine will affect this conjunct movement. 2) The back is flexed and thus it experiences high levels of stress placed on the discs (especially at the lumbosacral junction). 3) The exercise does not have a lot of functional carry-over to sport or daily life – Have you ever known anyone to sit down and push 400 lbs of weight? My recommendation – Train functionally in an upright position! 5) Knee Extensions 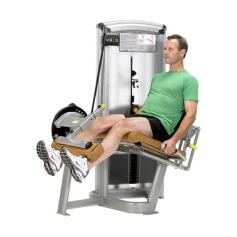 This machine is great for building quad mass, but is not great for the: 1) Patellofemoral Joint Arthrokinematics: (A) The way that the patella (knee cap) moves on the femoral condyles changes depending on whether you are performing an open or closed-chain exercise. Powers et al. (2003) found that the patellofemoral joint kinematics during non-weight-bearing (open chain) exercises could be characterized as the patella moving on the femur, while the kinematics during weight-bearing (closed chain) exercises could be characterized as the femur rotating underneath the stable. The latter of the two conditions provides the least amount of stress placed on the patellofemoral joint. (B) There is often additional stress placed on the patellofemoral joint because the load that you must push with your shin is anterior to the knee joint, whereas during a squat, the load is often through the knee joint or posterior to the knee joint. 2) Tibiofemoral Joint Arthrokinematics: For the same reason as explained in the leg press example above (#1), pushing your shin against the machine prevents some of the conjunct external rotation of the tibia on the femur, meaning that the joint mechanics may be dysfunctional and can lead to joint damage. 6) Back Extensions  This may be a good exercise to put on some erector spinal bulk, but over facilitation of this muscle group is already a common occurrence. Classically this facilitation occurs because of poor spinal stability via inhibited/weak deep core muscles (most significant = the multifidus muscles in this scenario). Performing this exercise may result in increased facilitation of the already facilitated erector spinae muscles. 7) Almost All Seated Exercises  Avoid almost all seated exercises, and especially ones that cause repeated lumbar rotation. The worst ones to avoid include exercises like the seated torso rotation machine, or any machines that force you into lumbar flexion (as mentioned above in #3). Remember Stuart McGills advice from above? The lumbar spine should be able to move dynamically, but have static stability when loaded. What i mean by this is that when the spine is not under any stress, we should have full range of motion through flexion, extension, rotation and side flexion. However, when loaded, the core muscles should provide stability and should remain static. If the spine moves when it is under load, additional shear and compression forces will occur, resulting in wear-and-tear on the spine. Lastly, when we must engage other muscle groups from a seated postion, we do not harness the stability and strength of the core. As a result we likely are weaker in that exercise, and we could be placing our body at risk for injury. Why? Because most sitting inhibits our ability to contract some of our core muscles (i.e. when sitting, the anterior abdominal cavity is compressed which inhibits the diaphragm from contracting), and some of our peri-core muscles (i.e. the glutes, hamstrings multifidi, erector spinae, etc. are lengthened and thus unable to contract as forcefully from the seated position). Concluding Remarks This is an interesting take on mobility that has helped me greatly: Always think about the body in terms of what should be mobile or stable. The following list will help to provide you with an understanding, and if applied correctly will help guide your training and any injury rehabilitation: Ankle — Mobile Knee — Stable Hip — Mobile Lumbar Spine — Stable Thoracic Spine — Mobile Scapula — Stable Glenohumeral — Mobile Remember that each joint should have full ROM regardless of its main purpose. Read more about this approach from Gray Cook’s book, 'Movement', ReferencesPowers, C.M., Ward, S.R., Fredericson, M., Guillet, M., Shellock, F.G. (2003). Patellofemoral kinematics during weight-bearing and non-weight-bearing knee extension in persons with lateral subluxation of the patella: a preliminary study. Journal of Orthopaedic and Sports Physical Therapy: 33(11): 677 – 685.
Within the developed nations of the world, and on the topic of progress, Canada seems to always maintain the status of happy-mediocrity: Occasionally leading the pack, occasionally trailing behind, but most often hanging out, comfy-right-dab-smack in the middle! On the topic of primary disease prevention, Canada is currently in a state of ‘comfy’.  As with most pre-cursers to change, money (or the lack-thereof) has Canadian Health Policy makers starting to brain-storm. We all know that with the baby-boomer population reaching more advanced ages, healthcare costs are on the rise… and frankly there will just not be enough finances to adequately fund health care. In fact, as of 2011, seniors over the age of 65 represented just 14% of the population but were using 40% of hospital services in Canada, AND accounted for about 45% of all provincial and territorial government health spending (Canadian Institute for Health Information (CIHI) – Health Care in Canada, 2011: A Focus on Seniors and Aging). The question is, what can be done? I’m a physiotherapist, and obviously physical health and wellness is my niche. Here is my take. I’d like to start with the idea that ‘for human-beings, the expression of life is movement’. Another way to look at this idea would be to understand that movement is how all living-beings interact with their own environment. For example: #1) The small muscles that allow us to move our eyes, allow us to see the environment around us. #2) The muscles of our hand allow us to handle and manipulate objects, show affection, build a home, or a cook meal. Therefore, if you cannot move well, your physical, emotional, and mental health will suffer. The conclusion should be that being able to move well is in many ways like a medicine – it can create positive changes in our health.  Unfortunately, day-to-day life can catch up to us as we age, and as a result we have a tendency to develop stiffness, pain, and become de-conditioned. These small problems often start to develop into larger and noticeable movement dysfunctions, changing the way that you move, and changing your focus from enjoying life to fixing the indicator of physical dysfunction – pain. If normal movement cannot occur, the human body adapts to these changes; Our vascular health deteriorates (heart, lungs, brain), we do not excrete as many toxins (leading to increased prevalence of cancers), our bone density decreases (leading to osteoporosis and arthritis), etc., etc.. The bottom line is that if we don’t move as much as we should, our internal health seriously deteriorates. The answer to better health (either primary, secondary or tertiary prevention of diseases/disorders) must be an interdisciplinary approach. Family Physicians, Optometrists, Dentists, and specialized health practitioners advise their patients that routine check-ups are preventative in nature, and may help to ensure optimal health. While their services may be essential, many health concerns still go unrecognized, unaddressed, untreated, or do not received adequate follow-up. The American Physical Therapy Association’s House of Delegates has a position statement on annual check-ups expressing “All individuals should visit a physical therapist at least annually to promote optimal health, wellness, and fitness, as well as to slow the progression of impairments, functional limitations, and disabilities”. While the Canadian Physiotherapy Association does not yet have a position statement on this matter they have agreed to bring the matter to the CEO’s attention who will relay the idea to the Board of Directors. My opinion on the matter is this: (1) Physiotherapists have superior knowledge of anatomy, physical function and dysfunction, treating holistically, and also treating very specifically. (2) Physiotherapists develop more meaningful relationships with their patients than many other health professionals due to the additional time spent with their patients. This should allow for greater insight into current impairments and lead to a more timely physical diagnosis which can help correct current dysfunctions, decrease the negative effects of a current diagnosis, and/or prevent future dysfunction from occurring. (3) This means added time at a lower cost, which provides greater value for the patient: More time for assessment, treatment, and follow-up. (4) Physiotherapy has can reduce risk factors and/or treat the most common co-morbidities in Canada (e.g. heart disease, diabetes, obesity, chronic disease). (5) Patients can benefit from physiotherapy at any age in terms of development, health promotion and wellness, maintenance of health, and disease prevention. (6) Patients who are provided with consistent and competent medical attention decrease or delay future health problem severity, maintain their quality of life for longer, and decrease the future financial burden on the public healthcare system.  93 year-old retired Dentist, Charles Eugster, dabbles in bodybuilding and rowing. So what is the drawback? Here are a select few:
(1) This service is currently advertised by a minority of physiotherapists in Canada – The general public does not even know this is an option! (2) Even if the general public had awareness, the expectations of the 21st century seem that if something is hard to achieve or attain, its not worth the initial effort. (3) Only a minority of people in Canada have benefit coverage for physiotherapy, and private physiotherapy services cost money. How many people in Canada are actually willing to pay out-of-pocket to help themselves when they are not in acute pain? The funding needs to be driven provincially/federally, or through private insurance. Suggestions for physiotherapists: Create a sample assessment of what should be included in an Annual Physiotherapy Assessment. Include a full body screen – put your neuro, cardioresp, AND MSK skills to use. Start advertising it and explain the benefits! Lobby your local physiotherapy association to increase interest in the matter! Suggestions for other readers: Find a therapist that specializes in Annual Physiotherapy Assessments and preventative health. Get an assessment and live a healthier life! If you found your assessment helpful, spread the news to your significant others! |
Have you found these article to be informative, helpful, or enjoyable to read? If so, please visit my Facebook page by clicking HERE, or click the Like button below to be alerted of all new articles!
Author
Jacob Carter lives and works in Canmore, Alberta. He combines research evidence with clinical expertise to educate other healthcare professionals, athletes, and the general public on a variety of health topics. Archives
November 2022
Categories
All
|


 RSS Feed
RSS Feed