
|
Recovering from an injury can be a nuanced process - there are some symptoms that you should listen to and others that aren’t so important, poor information abounds during searches on Dr. Google, there are friendly recommendations to try certain products, drugs or stretches, and just when you think it is okay to resume your normal activities pain may re-surge. It can be confusing… That being said, if you focus your attention on the overarching principles of an effective rehab, recovery doesn’t have to be complicated! Here are few key areas that anyone can assess and will help to simply your return to wellness: 1. Time  A) If you’ve sustained an injury, rehab will take time. Determining its severity can help you plan your rehab timeline. If it’s a small injury (micro-tearing or grade 1 sprain/strain), allow three days of relative rest for the injured area and slowly start to return to your sport. If it was a moderate or severe injury (grade 2-3 sprain / strain, fracture), you will need more time to allow the injury’s wound margins to heal back together. Due to the magnitude of a more severe injury you will likely benefit from a support (see below) and clever ways of modifying activity/programming. B) If you are not seeing many signs of improvement from your injury within a week, consulting a health care provider (Physio/Doctor) is a good idea. Diagnosing the injury and its severity will be important for your rehab strategy and long-term success. 2. Exercise  A) Make sure that you perform exercises specific for your injury/dysfunction. Your exercises should address all three of the following:
3. Supports  A) Your recovery from an injury may be uncomfortable but it needn’t be exquisitely painful. Utilizing walking aids (crutches/cane/walking poles), braces, taping techniques, medication (oral, topical or injections) or certain types of shoes/orthotics may help to alleviate some of your pain. These supports are not be relied on for very long, but can help reduce the harmful effects of feeling too much pain during your recovery. 4. Activity level  A). Many of my clients see me because they have slow progress or are seeing no progress. This is often because #2 is not being addressed and clients are often doing too much or too little activity in their day to day life. Determining the appropriate amount of activity requires:
Concluding Remarks Creating a good rehab program is an art. Of course there are other items to consider whilst recovering from an injury, but if you can dial in these four key areas it should help with setting realistic expectations and executing a planned recovery.
As always, if you have any questions feel free to send me an email or leave a comment!
2 Comments
As written for www.one-wellness.ca We try to improve the body’s natural response to injury in many different ways. Health professionals around the world offer products and techniques that promise the greatest reduction in inflammation and swelling, believing that their product can rise above the competition… But why?  Is it helpful to alter these responses, and is it even possible that we can alter these responses? For the most pragmatic answers, we can rely only on research… Definitions Understanding the differences in medical terminology allows us to better understand what processes are happening in our body. With this higher level of understanding, both practitioners and patients can better communicate what is happening in the body to achieve optimal outcomes. Swelling and inflammation of are often thought of as synonymous terms, however they have distinct definitions and applications. Inflammation: Inflammation is “a local response to cellular injury that is marked by capillary dilatation, leukocytic infiltration, redness, heat, and pain and that serves as a mechanism initiating the elimination of noxious agents and of damaged tissue” (1). 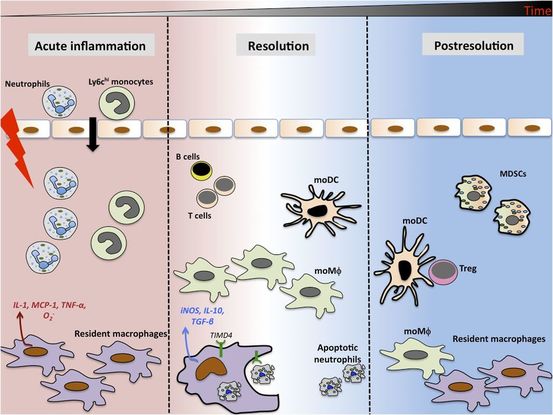 Cellular Inflammation Swelling: From Greek, the word ‘oídēma’ translates to ‘swelling’ (2). ‘Edema’ suggests “an abnormal infiltration and excess accumulation of serous fluid in connective tissue or in a serous cavity” (3).  Ankle Edema To briefly summarize, inflammation is a cellular response to tissue injury and may result in swelling, however swelling can actually occur within the body without the process of inflammation. A few common examples of swelling occurring within the body, in the absence of inflammation include: Lymphedema (failure of lymphatic drainage system to circulate blood plasma, and immune system regulators), cerebral edema (accumulation of extracellular fluid in the brain), pulmonary edema (accumulation of extracellular fluid in the lung). A few common examples of swelling that occurs within the body with inflammation as the causation includes: Acute tissue injury (fractures, sprains, strains), dermatitis (inflammation of the dermis layer of the skin), thrombophlebitis (inflammation of vein due to a blood clot). 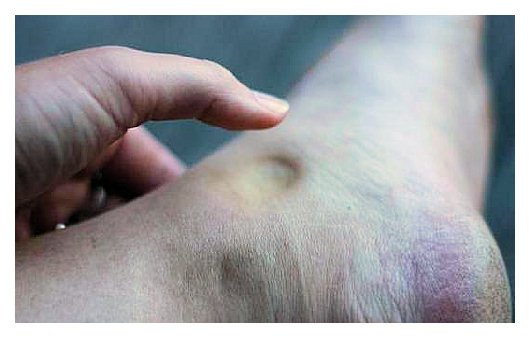 Classic presentation of pitting edema. While this may occur from thyroid conditions, pregnancy, salt-retention, heart failure, and some medication, I see it most frequently in clinic due to inflammation has not properly drained after soft-tissue injuries. Treating Inflammation Is it possible to alter the inflammatory response? Is it helpful to alter the inflammatory response? Over the last few decades there has been a culture of reducing inflammation immediately following acute injuries. However recent research has been changing the way clinicians should treat acute injuries: Anti-inflammatory medication can decrease the inflammatory response, but they may impair healing: In addition to their potential side effects (affecting GI tract, kidneys and cardiovascular systems), using NSAIDs (Non-steroidal anti-inflammatory drugs) may result in: a) Impaired bone healing after a fracture (4-9). b) Impaired tendon healing after an acute injury (10-11). c) No improvements in chronic tendinopathies, as there is no active inflammatory process (12). d) No improvement or possible small improvements in functional recovery In acute ligament injuries (13-18). Although one study found that using NSAIDs resulted in decreased pain and improved functional status, they also found a greater risk of adverse affects compared to using only analgesics. Also, one review of the literature found that acetaminophen is as effective as NSAIDs for pain reduction after musculoskeletal injury (19). These new results teach a few lessons: 1) The inflammatory mediators (e.g. prostaglandins, and cytokines) in inflammation help to initiate the subsequent stages of healing. 2) Removal of inflammation from an acute injury may harm the subsequent stages of healing. 3) In many cases, acetaminophen (e.g. Tylenol) will help to reduce pain as much as the use of anti-inflammatory medications, and will not impair healing. The overall justification for the use of the RICE principle (Rest, Ice, Compression Elevation) is very practical and helps minimize bleeding into the injury site. However, there has not been a single randomized, clinical trial to validate the effectiveness of the entire principle. 50 There is some support for each item, including immediate rest, and elevation to help in managing the accumulation of interstitial fluid (20). Summary: As much as possible restrict the usage of NSAIDs, employ the RICE principle, and if pain requires additional control then consider the use of other analgesic medications (e.g. acetaminophen, opiods, etc). It is a counterproductive goal to attempt to resolve all inflammation around the acute injury site. Treating Swelling Is it possible to alter swelling caused by acute injuries? Is it helpful to alter the swelling? It is possible to alter swelling that has been caused by acute injuries. In the following photos you can see that with appropriate rehabilitation, swelling improves. Unlike inflammation, it is in your best interest to reduce the amount of swelling at the local injury site. Depending on the amount of swelling, it can result in nerve compression, and restricted joint mobility making it painful and difficult to move the affected area (21). There is no benefit of allowing this swelling to stagnate as it will increase the level of irritability of the injury site and cause further deconditioning. While there are numerous modalities that purport to increase blood flow (e.g. interferential current, acupuncture, laser, ultrasound, etc., they majority lack substantial research and are unnecessary to resolve 99% of cases. In addition to the RICE principle mentioned previously, there are two supported methods to reduce swelling at the injury site: Movement - Regular movement of the affected joint, or at least the joints above and below should help pump the excess fluid back toward your heart using the lymphatic system. In addition, when able, start to perform cycling, swimming, rowing or perform upper body exercises. Massage - Stroking the affected area toward your heart using firm pressure may help move the excess fluid out of that area. There are many physiotherapists and massage therapists that have extra training in lymphatic drainage techniques that may be able to guide you, if you have been experiencing poor outcomes. References 1. Merriam-Webster Dictionary [Internet]. 2018. Inflammation; 2018-07-28. Available from: https://www.merriam-webster.com/dictionary/inflammation
2. Henry George Liddell, Robert Scott, A Greek-English Lexicon, on Perseus 3. Merriam-Webster Dictionary [Internet]. 2018. Edema; 2018-07-28. Available from: https://www.merriam-webster.com/dictionary/edema 4. Matsumoto MA, De Oliveira A, Ribeiro Junior PD, et al. Short-term administration of non-selective and selective COX-2 NSAIDs do not interfere with bone repair in rats. J Mol Histol. 2008;39:381-387. 5. Endo K, Sairyo K, Komatsubara S, et al. Cyclooxygenase-2 inhibitor delays fracture healing in rats. Acta Orthop. 2005;76:470-474. 6. O’Connor JP, Capo JT, Tan V, et al. A comparison of the effects of ibuprofen and rofecoxib on rabbit fibula osteotomy healing. Acta Orthop. 2009;80:597-605. 7. Bergenstock M, Min W, Simon AM, et al. A comparison between the effects of acetaminophen and celecoxib on bone fracture healing in rats. J Orthop Trauma. 2005;19:717-723. 8. Giannoudis PV, MacDonald DA, Matthews SJ, et al. Nonunion of femoral diaphysis: the influence of reaming and non-steroidal anti-inflammatory drugs. J Bone Joint Surg. 2000;82B:655-658. 9. Bhattacharyya T, Levin R, Vrahas MS, Solomon DH. Nonsteroidal antiinflammatory drugs and nonunion of humeral shaft fracture. Arthritis Rheum. 2005;53:364-367. 10. Elder CL, Dahners LE, Weinhold PS. A cyclooxygenase-2 inhibitor impairs ligament healing in the rat. Am J Sports Med. 2001;29:801-805. 11. Ferry ST, Dahners LE, Afshari HM, Weinhold PS. The effects of common anti-inflammatory drugs on the healing rat patellar tendon. Am J Sports Med. 2007;35:1326-1333. 12. Aström M, Westlin N. No effect of piroxicam on achilles tendinopathy: a randomized study of 70 patients. Acta Orthop Scand. 1992;63:631-634. 13. Lane LB, Boretz RS, Stuchin SA. Treatment of de Quervain’s disease: role of conservative management. J Hand Surg Br. 2001;26:258-260. 14. Dahners LE, Gilbert JA, Lester GE, et al. The effect of nonsteroidal antiinflammatory drug on the healing of ligaments. Am J Sports Med. 1988;16:641-646. 15. Moorman CT 3rd, Kukreti U, Fenton DC, Belkoff SM. The early effect of ibuprofen on the mechanical properties of healing medial collateral ligament. Am J Sports Med. 1999;27:738-741. 16. Ekman EF, Fiechtner JJ, Levy S, Fort JG. Efficacy of celecoxib versus ibuprofen in the treatment of acute pain: a multicenter, double-blind, randomized controlled trial in acute ankle sprain. Am J Orthop (Belle Mead NJ). 2002;31:445-451. 17. Ekman EF, Ruoff G, Kuehl K, et al. The COX-2 specific inhibitor Valdecoxib versus tramadol in acute ankle sprain: a multicenter randomized, controlled trial. Am J Sports Med. 2006;34:945-955. 18. Slatyer MA, Hensley MJ, Lopert R. A randomized controlled trial of piroxicam in the management of acute ankle sprain in Australian Regular Army recruits. The kapooka ankle sprain study. Am J Sports Med. 1997;25:544-553. 19. Feucht CL, Patel DR. Analgesics and anti-inflammatory medications in sports: use and abuse. Pediatr Clin North Am. 2010;57:751-774. 20. van den Bekerom MP, Struijs PA, Blankevoort L, Welling L, Van Dijk CN, Kerkhoffs GM. What is the evidence for rest, ice, compression, and elevation therapy in the treatment of ankle sprains in adults?. J Athlet Train. 2012 Jul;47(4):435-43. 21. Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J. Harrison’s Principles of internal medicine. New York: McGraw-Hill Companies. 18th ed; 2011. Although I've taken several courses that address concussion assessment and treatment over the last few years, research is continually advancing our knowledge of guidelines. Here is a summary I've put together of some of the most recent literature which aims to answer the questions: Which patients require concussion rehabilitation and what does recent evidence suggest that concussion rehabilitation should include?  Assessment and Treatment Timelines The most recent International Consensus Statement on Concussion in Sport (The Berlin Consensus Statement, April 2017) states that evidence-based treatment for persistent concussion symptoms includes cervical spine treatment, vestibular rehabilitation, psychological interventions, and controlled submaximal exercise (1). The diagnosis of a concussion is a clinical judgment, made by a medical professional (1). A multi-faceted treatment approach seems to be the most effective approach to rehabilitation, and should begin immediately by obtaining a comprehensive history, performing a neurological exam to rule out serious pathology related to traumatic brain injury (TBI) or vascular insufficiency, and screening the cervical spine for signs of trauma. As a minimum, the health care team involved in the patient’s care should include a Family Physician and/or Sports Medicine Physician, and a Physiotherapist trained in concussion management. As required, patients may also benefit from a referral to see a psychologist, optometrist or dietician trained in concussion management. Recent evidence suggests that starting rehabilitation as early as 10 days after injury improves recovery time and decrease the risk of developing post-concussion syndrome (PCS) (2). For individuals with PCS, a multifaceted assessment is needed to identify targeted treatments that may be of benefit (3). Cervical, Vestibular, and Oculomotor Rehabilitation The amount of force necessary to sustain a concussion is far greater than that which is needed to sustain a whiplash (4). As a result, nearly every concussion sustains a whiplash as well. The significance of this fact is that whiplash injuries can disrupt the vestibular system (causing dizziness and vision dysfunction), result in cervical joint and muscle tightness/inflammation (causing local pain, referred headaches, and contribute to a lack of concentration), and disrupt the reflexes between cervical-vestibulo-occular system. In 2014, Schneider et al., published one of the first randomized clinical trials comparing a group receiving a combination of cervical and vestibular rehabilitation versus a control group that was given the usual protocol of rest followed by gradual exertion. Both groups received treatment from a physiotherapist at least once per week for 8 weeks, and had an average age of 15 years. In the treatment group, 73% of the participants were medically cleared within 8 weeks of initiation of treatment, compared with 7% in the control group. Individuals in the treatment group were 3.91 (95% CI 1.34 to 11.34) times more likely to be medically cleared by 8 weeks (2,5). In 2017, Reneker et al., published another randomized clinical trial comparing individualized treatment plans consisting of manual therapy of the neck, vestibular rehabilitation, oculomotor and neuromotor retraining, to a control group. Subjects were permitted by a sports medicine physician to enroll in the trial if they had experienced concussive symptoms for at least 10 days, and were treated by a Physiotherapist for up to a maximum of 8 visits or until they were fully cleared to return to play by a blinded sport-medicine physician. The progressive treatment group achieved symptom resolution and clearance to resume full sport activities significantly sooner than the control group: 15.5 days versus 26 days, respectively. The authors concluded that a personalized treatment plan beginning as early as 10 days after concussion may be an effective option to shorten recovery time (6).  Exercise Recommendations Post-Concussion Initiating physical activity within the first 7-14 days post-concussion has been associated with a decreased risk of developing PCS. These results have been noted in adolescents and adults (7-12). Several clinical trial have demonstrated significant improvements in symptoms, cerebral blood flow mechanics, and complete return to all pre-injury activities over a much faster timeline compared to control groups or sham therapies (i.e. stretching). This is true for both acute concussions and PCS (7-10). Research would suggest performing low-level aerobic exercise most days of the week, at 80% of their symptom-tolerated heart rate (13,14). Summary: Providing Effective Treatment In addition to a graduated ‘Return to Learn’, ‘Return to Work’, and/or ‘Return to Play’ protocol, patients recovering from concussions seem to benefit the most from specific therapies for the cervical spine, vestibular system, visual system, and cardiovascular system. Research suggests that focused rehabilitation that begins within the first 7 to 10 days after injury can significantly improve outcomes and decrease long-term symptoms in both children and adults. References 1) McCrory P, Meeuwisse W, Dvorak J, Aubry M, Bailes J, Broglio S, Cantu RC, Cassidy D, Echemendia RJ, Castellani RJ, Davis GA. Consensus statement on concussion in sport—the 5th international conference on concussion in sport held in Berlin, October 2016. Br J Sports Med. 2017 Apr 26:bjsports-2017.
2) Schneider K, Meeuwisse W, Nettel-Aguirre A, Boyd L, Barlow KM, Emery CA. Cervico-vestibular physiotherapy in the treatment of individuals with persistent symptoms following sport-related concussion: a randomized controlled trial. Br J Sports Med. 2014 May 1;48:1294-8. 3) Feddermann-Demont N, Echemendia RJ, Schneider KJ, Solomon GS, Hayden KA, Turner M, Dvořák J, Straumann D, Tarnutzer AA. What domains of clinical function should be assessed after sport-related concussion? A systematic review. Br J Sports Med. 2017 Jun 1;51(11):903-18. 4) Marshall CM, Vernon H, Leddy JJ, Baldwin BA. The role of the cervical spine in post-concussion syndrome. The Physician and sportsmedicine. 2015 Jul 3;43(3):274-84. 5) Schneider KJ, Meeuwisse WH, Barlow KM, Emery CA. Cervicovestibular rehabilitation following sport-related concussion. Br J Sports Med. 2018 Jan 1;52(2):100-1. 6) Reneker JC, Hassen A, Phillips RS, Moughiman MC, Donaldson M, Moughiman J. Feasibility of early physical therapy for dizziness after a sports‐related concussion: A randomized clinical trial. Scand J Med Sci Sports. 2017 Dec 1;27(12):2009-18. 7) Baker JG, Freitas MS, Leddy JJ, Kozlowski KF, Willer BS. Return to full functioning after graded exercise assessment and progressive exercise treatment of postconcussion syndrome. Rehab Res Pract. 2012. 8) Leddy JJ, Cox JL, Baker JG, Wack DS, Pendergast DR, Zivadinov R, Willer B. Exercise treatment for postconcussion syndrome: a pilot study of changes in functional magnetic resonance imaging activation, physiology, and symptoms. J Head Trauma Rehab. 2013 Jul 1;28(4):241-9. 9) Gagnon I, Grilli L, Friedman D, Iverson GL. A pilot study of active rehabilitation for adolescents who are slow to recover from sport- related concussion. Sci and J Med Sci Sports. 2015; 26(3):299–306. 10) Imhoff S, Fait P, Carrier-Toutant F, Boulard G. Efficiency of an active rehabilitation intervention in a slow-to-recover paediatric population following mild traumatic brain injury: a pilot study. J Sports Med. 2016. 11) Lal A, Kolakowsky-Hayner SA, Ghajar J, Balamane M. The Effect of Physical Exercise after a Concussion: A Systematic Review and Meta-Analysis. Am J Sports Med. 2017 Jun 1. 12) Zemek R, Grool AM, Aglipay M, Momoli F, Meehan WP, Freedman SB, Yeates KO, Gravel J, Gagnon I, Boutis K, Meeuwisse W. Relationship of early participation in physical activities to persistent post-concussive symptoms following acute paediatricpediatric concussion. Br J Sports Med. 2017 Jun 1;51(11):A20. 13] Schneider KJ, Leddy J, Guskiewicz K, Seifert TD, McCrea M, Silverberg N, Feddermann-Demont N, Iverson G, Hayden KA, Makdissi M: Rest and specific treatments following sport-related concussion: A systematic review. Br J Sports Med. 2017 Mar 24, 51:930-4. 14) Leddy JJ, Kozlowski K, Donnelly JP, Pendergast DR, Epstein LH, Willer B. A preliminary study of subsymptom threshold exercise training for refractory post-concussion syndrome. Clin J Sport Med. 2010 Jan 1;20(1):21-7 Basics of Tendon Function Tendons attach muscles to bones. Simple enough, right? Well... kind of... not really! 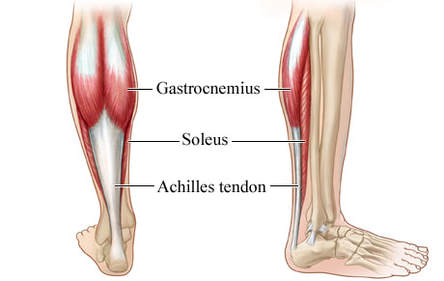 Our two largest calf muscles, the gastrocnemius and soleus are both connected to the calcaneus (heel bone) via the achilles tendon. Tendons are a specific type of force-transmitting architecture between a muscle and a bone. They are made of a strong fibrous collagen tissue and transmit the force of muscular contraction to a bone in an effort to create joint motion. Good quality tendons are like stiff springs; A stiff spring will stretch a little, and then recoil with most of the force that was required to stretch it initially. In our tendons, we call this stretch 'creep', and the recoil of the tissues 'recovery'. To prevent wasting energy and causing damage to a spring (or a tendon in this case), we need to have a certain degree of stiffness, resilience and efficiency. An example of this would be if I create tension in my calf by hopping on a single leg. The calf muscles transfer this fairly high load to my calcaneous bone via the achilles tendon. When I do this action repeatedly, a strong tendon will be able to handle the load that is asked of it... whereas a tendon with poor load tolerance may start to creep and not recover quickly... which means that some of the energy that was loaded into the tendon will be lost. This can lead to fatigue of the tissue, and eventually inflammation and micro or macrotearing of the tendon (small tears or a complete rupture). Peritendinous Dysfunction There are three common anatomical areas that lead to peritendinous dysfunction and pain: The weakest zones of a tendon are where it transitions from tendon to bone (enthesis), followed by the transition zone from muscle to tendon (musculotendinous junction) (1). 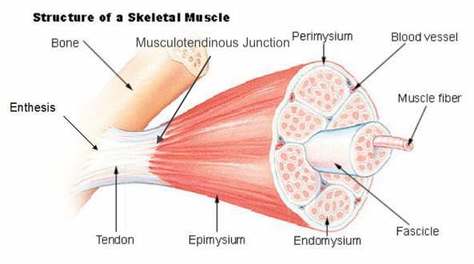 Transition from muscle to tendon to bone, with the musculotendinous junction and the enthesis noted in the photo Additionally, since tendons are mostly found near joints, they are protected from the hard bony surface by a bursa (a fluid-filled sac). If there is excessive compression of a tendon on a bursa, it will often become inflamed and irritable. This is more common than you'd expect, and often a diagnosed tendinopathy includes a bursitis.  This photo illustrates a few of the bursae located around the patella. Our body is designed such that any location where there is higher friction between two surfaces, a bursa will typically be present to provide padding and lubrication. Creating Tendon Irritability Tendons become irritable when they are stressed beyond their load tolerance. Overuse may develop for one of many reasons: 1) Excessive volume: Tendons may not be able to adapt to an increased volume of a specific activity (over a period of days/weeks/months) 2) Poor biomechanics: Doing a motion differently than you may have done it previously (over a period of days/weeks/months) may cause irritability, even if the volume hasn't changed. If you've been doing a specific motion with poor biomechanics for a while, but then increase the volume, re-read principle #1. 3) Impaired mobility or strength elsewhere: Often, a proximal or distal impairment may cause you to (a) move poorly, which may ultimately cause you to over use some parts of your body and under-use others (b) compress on nerve tissues 4) Excessive stretching: Prolonged and frequent stretching of muscles/tendons may result in excessive creep and poor recovery of the tendon. Subsequent loading of the tendon may result in increased potential of tendon irritation. 5) Nerve compression: Decreased space at the intervertebral foramen (where the nerves exit your spine), or compression of a nerve by tight muscles may affect the strength of the muscles supplied by that nerve. This may cause poor movement patterns, referred pain, and /or dysfunctional muscle tone that may cause irritation of the tendon. 6) Maintenance required: Even with reasonable volume and good biomechanics, if you ask your body to perform an activity enough and don't ensure that the muscles maintain good mobility and tissue quality, the muscles may develop trigger points which in turn will pull on its tendon with increased tension. 7) Intrinsic factors: An individual's risk for developing tendinopathy is also affected by older age, sex, and systemic diseases such as Marfan's Syndrome, Ehlers–Danlos Syndrome, thyroid disorders, diabetes, rheumatoid arthritis, and having a predisposition to developing kidney stones, gallstones or gout(2). Changes on a Cellular Level Microtearing of tendon fibers will evoke a cascade of events, mainly in areas with poor blood supply: 1) Cytokines (small proteins that have an effect on the behavior of cells around them) activate tendon fibroblasts (cells that help to lay down type 3 collagen to help with the initial healing the cellular matrix that was disrupted). 2) At the same time, pain stimulating mechanisms are activated due to the inflammation that was created during the activity that damaged the tendon. 3) Other proteins in the area stimulate enzymes that degrade the extracellular matrix (the support network for tendon cells), and promotes the formation of new blood vasculature and new nerves (3).  Yup, this thickened tendon is actually at greater risk of tearing or rupture. It is thicker because of excess inflammation and water, excessive production type 3 collagen fibers and misalignment of the type 3 collagen fibers. The result is a thicker, yet weaker tendon. It has a greater density of nerve endings which increases the sensitivity to all stimuli including the chronic inflammation. Together, these factors create a positive feedback system in which the inflammation irritates the nerve endings, causing increased inflammation... AND the chronic inflammation degrades the quality of the tendon itself. This means that when the tendon is loaded during sports or daily activities, further injury will occur to the tendon, thus creating additional inflammation and pain (3). 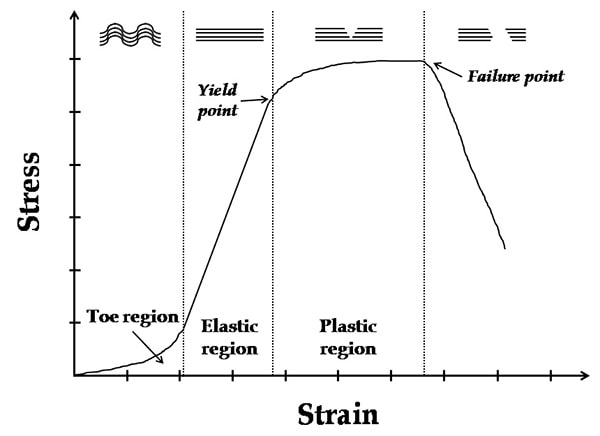 When a tendon is loaded or stretched beyond the elastic range, it experiences irreversible creep (plastic changes) to the tissue. This is known as microtearing, and will eventually lead to collagen / scar tissue formation, resulting in tendon thickening. If it continues beyond the plastic phase, macrofailure (a complete tear) of the tendon may occur (4,5). Tendon Take-Homes Statistically significant increases in tendon strength can be seen in the research after approximately 2-3 months of consistent strength training. Conversely, in a prolonged period of deloading, it only takes between 2-4 weeks to see statistically significant decreases in tendon strength (6-8). Therefore, a few general principles can be gleaned from all of the above information: 1) Train regularly, and do not take more than 2 weeks off from strength training, or else you may face the consequences. 2) Gradually increase your training volume in anything you do that is physically active. 3) Correct the mobility restrictions, strength impairments, and poor movement patterns that are within your control. Have a good personal trainer, coach, or physiotherapist assess your movement patterns. 4) If you are using your body regularly, use a foam roller regularly (poor man's massage therapist), and see a body worker (e.g. massage therapist or physiotherapist) for maintenance visits (once a month minimum). 5) Control your modifiable risk factors for developing comorbid conditions: Eat (mostly) healthy, sleep (mostly) well, and live a happy and stress-reduced life. Stay tuned for my next article that will examine elbow tendinopathy and management strategies! References 1) Apostolakos J, Durant TJ, Dwyer CR, Russell RP, Weinreb JH, Alaee F, Beitzel K, McCarthy MB, Cote MP, Mazzocca AD. The enthesis: a review of the tendon-to-bone insertion. Muscles, ligaments and tendons journal. 2014 Jul;4(3):333.
2) Rees JD, Wilson AM, Wolman RL. Current concepts in the management of tendon disorders. Rheumatology. 2006 Feb 20;45(5):508-21. 3) Abate M, Silbernagel KG, Siljeholm C, Di Iorio A, De Amicis D, Salini V, Werner S, Paganelli R. Pathogenesis of tendinopathies: inflammation or degeneration?. Arthritis research & therapy. 2009 Jun;11(3):235. 4) Svensson RB, Hassenkam T, Hansen P, Magnusson SP. Viscoelastic behavior of discrete human collagen fibrils. Journal of the Mechanical Behavior of Biomedical Materials. 2010 Jan 1;3(1):112-5. 5) Ryan ED, Herda TJ, Costa PB, Walter AA, Hoge KM, Stout JR, Cramer JT. Viscoelastic creep in the human skeletal muscle–tendon unit. European journal of applied physiology. 2010 Jan 1;108(1):207-11. 6) Kubo K, Ikebukuro T, Maki A, Yata H, Tsunoda N. Time course of changes in the human Achilles tendon properties and metabolism during training and detraining in vivo. Eur J Appl Physiol. 2012;112:2679–91. 7) Kubo K, Ikebukuro T, Yata H, Tsunoda N, Kanehisa H. Time course of changes in muscle and tendon properties during strength training and detraining. J Strength Cond Res. 2010;24:322–31. 8) de Boer MD, Maganaris CN, Seynnes OR, Rennie MJ, Narici MV. Time course of muscular, neural and tendinous adaptations to 23 day unilateral lower-limb suspension in young men. J Physiol. 2007;583:1079–91 While manual therapy and education may play a crucial role in injury rehabilitation, injuries and pain respond the best in the long-term to progressive loading through exercise. In fact, exercise is said to be "the closest thing to a miracle cure" (1), and is widely accepted as the means through which you can attain complete recovery. Prescribing exercise can be intimidating for some therapists, so I wanted to provide some facts and guidelines that may help make this easier!  Fitting the Diagnosis to the Injury Attaining an accurate diagnosis CAN be difficult, but is often the first stage to developing a treatment plan, including exercise. 1. Do we know the actual pathology/diagnosis? An over-reliance on imaging and unreliable ‘special’ tests may mean that the true pathology (AKA reason for the client’s pain) may not fully be understood. A) Imaging typically looks at the injury site at a specific moment in time. To develop a true understanding of the pathology, this information must be examined along with the patient's subjective history and movement patterns. A common example in knee pain would be that an x-ray finding of moderate osteoarthritis of the patella is an additional finding, when the true reason for the patient's knee pain is trigger points in the quadriceps caused by suboptimal movement control. B) Many Special Tests are not that special. A special test should look to confirm suspicions of a specific diagnosis - they should not be used initially when developing a diagnosis. We know that many special tests lack sensitivity and specificity, and as a result are not helpful in confirming the diagnosis (even with a proper history and objective exam). Nicklaus Biederwolf, a physiotherapist and researcher, has this to say about special tests specific to the shoulder: "A great lack of consistency with regard to how, when, and what special tests to use in clinical examination for shoulder differential diagnosis is evident" (2). C) Different health care practitioners may develop different diagnoses that fit the information gathered during their assessment, and their bias. It is important to do a comprehensive assessment (including the client's previous medical history, mechanism of injury, pattern of pain, global movement patterns, and a specific joint/tissue/nervous system/vascular assessment). 2. Without imaging, we depend on clinical patterns to develop an accurate diagnosis, however similar pathologies may behave differently in the clinical setting. For example a partial thickness supraspinatus tear (one of the shoulder's rotator cuff muscles) may behave differently in one client versus other clients - and this may be for a wide variety of reasons: A) Anatomical variations: The acromion (a protrusion on our shoulder blade, under which the supraspinatus tendon glides) come in all shapes and sizes. The same applies to the rest of our bones, and muscles/tendons in our body - we are not as symmetrical and standardized as you may think! B) Regional Interdependence: Canadian Physiotherapists are known as 'The Movement Specialists' (3), so keep connecting the dots to determine how one area of the body may be affecting another! The thoracic spine, neck, scapula and all of its connecting muscles and ligaments alter the dynamic control and posture of the shoulder, which ultimately impact the supraspinatus tendon. C) Variations in nociception (sensing pain): Fewer pain nerve endings near the injury site, previous injury to nerve or blood supply at the area, or differences in central nervous system perception of pain on a global level will affect how a patient feels potentially harmful stimuli. D) Multiple injuries: A mechanism of injury that may tear the supraspinatus may also injure other tissues in the area. For example, there could also be an injury of the labrum, chondral surface of the humerus, biceps tendon, pec major, or subacromial bursa. It is nearly impossible to identify/distinguish all of these pathologies in the clinic without imaging... BUT does it really matter? Read on! What To Do.. in a World of Unknowns? It can all get quite confusing.. The items above paint a muddled picture: It can be quite difficult to come up with the correct diagnosis due to many(!!!) factors. Luckily, despite this fact, there are a few things we can do that will promote successful recovery. 1. It may be more important to focus on movement deficits first. Our bodies are exceptional at healing themselves. In fact, the best athletes in the world are the ones that recover the quickest (from training, games, or injuries). Most of the time, the injured tissue will heal on their own, but will leave us with tight muscles and poor movement patterns as a result of compensation. This means that pursuing imaging and specialist appointments may just end up being a waste of time, health care dollars, and stress. To start, the patient shoulder obtain a couple of opinions (physician and physiotherapist) to determine whether medical testing may be needed. Following these opinions, it is usually best to focus on improving flexibility and movement control. 2. Zoom out; Broaden your perspective! Often we warn patients against performing certain exercises, based on the fact that they have a certain pathology (e.g. with an acute partial tear of the supraspinatus tendon, stay away from dips or deep bench press). Take a step back and look at global movement patterns - are there any other restrictions / dysfunctions that you could work on first? In our case example: Do you need to work on thoracic mobility, activating scapular upward rotators, releasing scapular downward rotators, activating deep neck flexors, releasing posterior rotator cuff, releasing adhesions at the interface of pec major / supraspinatus / long head of biceps? Maybe a further step back would even suggest asymmetries in lower body, lower back, or neck strength/mobility. 3. Prescribing the exercise. Suggesting that the patient does a specific exercise is not enough. Ensure that the correct exercise is performed correctly; Spend time on coaching form and don’t expect that your client knows how to do the exercise properly. Lastly, discuss the importance of correct exercise: 1. Volume 2. Intensity 3. Rest 4. Tempo By changing these four variables, we can ultimately train the tissue work for its intended purpose and improve A) Muscular endurance B) Muscular power C) Muscular reactivity (plyometrics) D) Tendon loading capacity 4. Test, and Re-Test If you've taught the exercises well, allow adequate time for a beneficial result to occur, and re-test the client's functional deficits. 5. Lastly, a client’s most effective exercises may change overtime due to movement quality, tissue quality, perceived effort/challenge, ability to recover quickly, or the applicability to sport and life specific challenges. Follow up a few weeks or months down the road to provide the best possible care to your client.  References (1) Academy of Medical Royal Colleges. Exercise: The miracle cure and the role of the doctor in promoting it. AOMRC.org.uk. 2015 Feb
(2) Biederwolf, Nicklaus E. "A proposed evidence-based shoulder special testing examination algorithm: clinical utility based on a systematic review of the literature." International journal of sports physical therapy 8.4 (2013): 427. 3) Physiotherapy Alberta: About Physiotherapy. Accessed February 1, 2018. https://www.physiotherapyalberta.ca/public_and_patients/about_physiotherapy |
Have you found these article to be informative, helpful, or enjoyable to read? If so, please visit my Facebook page by clicking HERE, or click the Like button below to be alerted of all new articles!
Author
Jacob Carter lives and works in Canmore, Alberta. He combines research evidence with clinical expertise to educate other healthcare professionals, athletes, and the general public on a variety of health topics. Archives
November 2022
Categories
All
|


 RSS Feed
RSS Feed